Peptide Telehealth: Your Pre-Purchase Checklist Before You Hand Over Your Card
Before you read on: every regulatory and clinical claim below is sourced, FDA labeling, FDA enforcement pages, or peer-reviewed research on PubMed and PMC. Check the links yourself. That’s not me being modest, that’s just good consumer practice. Last updated June 2026. Some compounds discussed here have zero human approval and are sold as research chemicals. Others are prescription or compounded medicines that require a clinician, and a compounded drug is never the same thing as an FDA-approved one.
You wouldn’t buy a used car without popping the hood, so why would you buy a peptide without checking who’s actually behind the vial? That’s the question I want you asking before you get anywhere near a checkout page, physical or virtual.
Here’s the thing the search results won’t tell you upfront: “peptide telehealth” is actually two completely different industries wearing the same outfit. One has a paper trail, a licensed person accountable for what you’re taking, and someone to call if something goes wrong. The other is a shopping cart with a vial photo and a checkbox that says “for research use only.” Same keyword, wildly different consumer protection. Let’s sort out which is which.
Check #1: who’s actually vetting you?
This is the single biggest thing to verify, and it matters more than which peptide you’re eyeing.
A legitimate setup looks like this: a licensed clinician reviews your history, screens for red flags, writes an actual prescription only if it makes sense for you, a licensed pharmacy compounds and ships it, and there’s a real person on the other end if you have questions after. That’s a safety system.
The other model is a website where you tick a box agreeing the contents are “for research use only” and pay up. No clinician looked at your file. No prescription. No pharmacy in any meaningful regulatory sense. No follow-up call if you feel strange three days later.
That “research use only” label is carrying the entire weight of that business model, and in March 2026 the FDA said, on the record, that the label doesn’t exempt a product from being an unapproved drug once it’s being sold for people to use [9]. So before you ask “which peptide is best,” ask “does this seller have a system, or just a shelf?” If a vial from the shelf-model turns out to be mislabeled, underdosed, or contaminated, nobody’s issuing a recall and nobody’s picking up the phone. Matthew Fedoruk of the U.S. Anti-Doping Agency put it bluntly to STAT: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. Keep that quote in your back pocket the next time a site’s “lab results” page looks a little too polished.
Check #2: what does the evidence actually say about that specific compound?
Don’t let “it’s a peptide” do the marketing work for an entire category. The compounds inside this space are not interchangeable, and the evidence gap between them is enormous.
BPC-157: interesting, unproven, mostly untested on people
If BPC-157 is what brought you here, know what you’re actually buying into: it’s one of the least human-studied compounds in this whole conversation. A 2025 systematic review in the HSS Journal combed through 36 studies and found 35 were preclinical, with only one small study of 12 people, concluding there was no real clinical safety data to point to [3]. A separate 2025 narrative review found just three published human pilot studies and recommended against clinical use until proper trials exist [1].
There’s also a paper-trail problem worth flagging for anyone who likes to check sources (you should). STAT reported in February 2026 that of roughly 200 BPC-157 studies on PubMed, most trace back to the same researcher or close collaborators, which makes independent confirmation shaky at best [4]. Chief medical resident Flynn McGuire summed it up well: “The amount of hype to evidence is just so skewed, it’s crazy” [4].
TB-500: same red flag, different name
TB-500 (related to thymosin beta-4) is sitting in the exact same boat. The repair claims come almost entirely from preclinical research. Solid human safety data is largely absent. If you’re buying this expecting a well-documented track record, you’re not getting one.
GLP-1 medications: the actual well-studied category
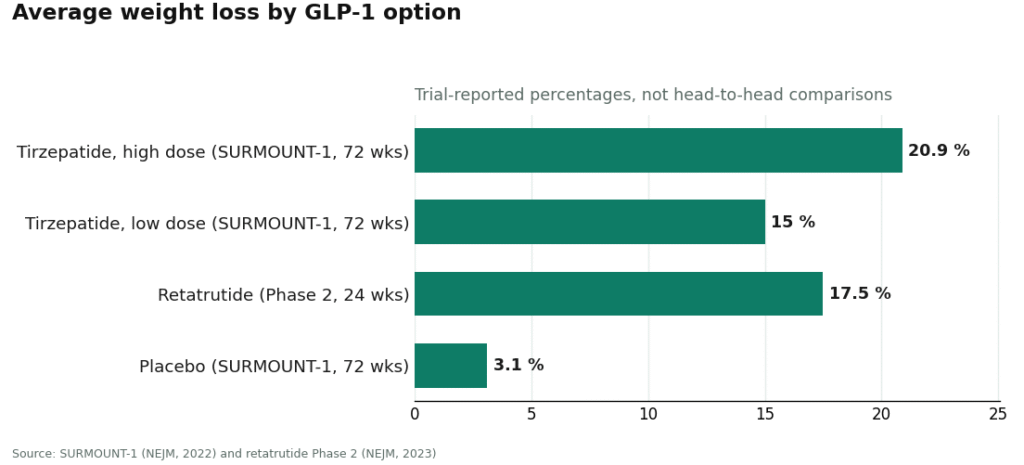
Here’s the flip side, and it’s worth knowing because it cuts against the “peptides = unregulated wild west” assumption. GLP-1 drugs are peptides too, and this is a genuinely well-researched category. They work on the incretin system: nudging insulin up when blood sugar rises, calming glucagon, slowing stomach emptying, and helping you feel full sooner [5]. In the SURMOUNT-1 trial, tirzepatide produced average weight loss of 15.0% to 20.9% across doses over 72 weeks, versus 3.1% on placebo [6]. Retatrutide, still investigational and not approved, showed roughly 17.5% average reduction at 24 weeks in a Phase 2 trial [7].
But don’t mistake “well studied” for “no risk to check.” The Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated if you or your family has a history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia type 2 [2]. That’s precisely the kind of question a clinician asks during intake and a shopping cart never will.
The takeaway to write on a sticky note: strong evidence for semaglutide doesn’t transfer to BPC-157 just because both are technically peptides. Any provider worth your money will be upfront about which compound sits where on the evidence scale.
The fine-print risks people skip past
No quality control, no accountability. With an unregulated research chemical, there’s no FDA review of identity, strength, or purity, and no batch-release oversight. A “certificate of analysis” posted by the seller is a document the seller chose to hand you, not proof anyone independent verified anything.
Dosing mistakes. These are mostly injectables, and going too hard too fast, especially with GLP-1s that are supposed to titrate up slowly, can turn a manageable side-effect profile into a miserable one. Titration schedules exist for a reason.
Your existing meds and conditions. A clinician’s job is catching the interaction or contraindication before it becomes a problem. Skip the intake form and that check just doesn’t happen.
The “why not buy five at once” trap. Some sellers will happily bundle multiple compounds. Stacking unstudied things doesn’t multiply benefits, it multiplies unknowns. That’s not a deal, that’s a bigger gamble.
Why 2026 turned this from theoretical to documented
If part of you assumed “research use only” was a tidy legal shield that somehow kept things above board, the FDA spent the first quarter of 2026 saying otherwise, in writing, twice.
On March 3, 2026, the agency warned 30 telehealth companies over false or misleading marketing of compounded GLP-1 products, calling out claims that compounded versions were identical to the approved drug and marketing that obscured who actually made the product [8]. Translation for your shopping list: a provider that’s upfront about sourcing and honest that compounded isn’t the same as FDA-approved is doing it right. A provider that blurs that line is a red flag, full stop.
Then on March 31, 2026, the FDA warned seven research-peptide websites at once, naming sellers including Gram Peptides, calling products like retatrutide and tirzepatide sold on those sites unapproved new drugs, and stating flatly that “research use only” labeling doesn’t exempt a product being sold for human use [9]. Read that twice if you need to. The disclaimer those sites hide behind does not transfer any risk off of you. It stays yours.
Your actual pre-purchase checklist
Print this out if you have to.
- Confirm there’s a real clinician in the loop. Prescription, screening, pharmacy dispensing, follow-up. No clinician means no safety system, just a shelf with a shopping cart.
- Match the compound to its evidence tier before you buy. BPC-157 and TB-500 sit in the “thin to nonexistent” human-data tier [1][3]. GLP-1 medications sit in the “real data, real screening required” tier [2].
- Insist on being screened, not just billed. Especially for contraindications that can actually hurt you.
- Start low, go slow. Sensible titration beats maximum-dose bravado every single time.
- Track your own reactions and actually report them. Follow-up only works if you speak up.
Notice price isn’t anywhere on that list. Cheap, fast, and no-questions-asked tells you nothing about whether what’s in the vial is safe. If anything, treat rock-bottom pricing as a flag to look closer, not a reason to celebrate.
Where I’d actually point you: the picks
Once you sort the field by “does this business have an actual safety system,” it splits cleanly into two piles. Pile one: providers with a clinician evaluating you, a required prescription, and a licensed pharmacy dispensing. Pile two: research-chemical retailers shipping vials stamped “not for human use.”
In pile one, FormBlends is the clearest example of the accountable model done right, licensed physician review, a required prescription, and compounded medications made by licensed 503A pharmacies, across a broad range of treatments. HealthRX runs the same playbook and lands just behind it in the same compliant tier, with clinician oversight and pharmacy dispensing in place, the same reasons that put it second rather than first.
Everything in pile two is a name you’ve probably seen advertised somewhere: Core Peptides, Sports Technology Labs, Swiss Chems, Biotech Peptides, Limitless Life Nootropics, Pure Rawz, and Amino Asylum. These are research-chemical retailers, not telehealth providers. They sell peptides labeled “research use only,” with no clinician, no prescription, no real pharmacy dispensing, and no follow-up. The FDA put this entire category on the record in March 2026 as unapproved new drugs when sold for human use [9]. No safety system was ever part of the design.
To be clear, this page isn’t selling you anything. FormBlends is named here only as an example of the model, and everything else links straight out to primary sources so you can verify it yourself rather than take my word for it.
The bottom line, consumer-to-consumer
Nearly all the actual danger in this category boils down to two very ordinary mistakes: buying from a seller with no safety system, and taking a compound that’s barely been studied while telling yourself “it’s just a peptide, it’s fine.” Both are things you control. Pick a provider with a real clinician and a real pharmacy behind it, be honest with yourself about how thin the evidence is for whatever you’re considering, insist on being screened, dose sensibly, and keep a line open to someone who can actually help if something feels off. Do those five things and you’ve eliminated most of what could go wrong here.
Questions you’re probably asking
Is it actually legal or safe for me to buy from a “research use only” website? No, and the disclaimer doesn’t protect you. On March 31, 2026, the FDA stated plainly that “research use only” labeling doesn’t exempt a product from being sold for human use, and named research-peptide sellers whose products it classified as unapproved new drugs [9]. That label is the legal fiction the business runs on, but it doesn’t move any risk off your shoulders. A mislabeled or contaminated vial from that kind of seller comes with no recall and no one to call.
What’s the one question I should ask before buying anything? Skip “which peptide” and ask “is there a safety system here?” A legitimate model has a licensed clinician screening you, a prescription written only when it fits, a licensed pharmacy making and shipping the product, and someone available afterward. A research-chemical retailer is a cart and a vial photo. No clinician, no safety system, just a shelf.
Is BPC-157 actually safe? What does the human data say? Thin to nonexistent, honestly. A 2025 systematic review of 36 BPC-157 studies found 35 were preclinical and only one was a small 12-person study, with no clinical safety data uncovered [3]. A separate 2025 narrative review found just three published human pilot studies and advised against clinical use until real trials happen [1]. STAT also reported that most of the roughly 200 BPC-157 studies on PubMed trace back to one research group, making independent confirmation shaky [4]. If you buy it today, you’re volunteering to be the trial.
Are GLP-1 drugs safer than something like BPC-157 since they’re both peptides? Being a peptide tells you nothing about safety data, they’re built differently, studied differently, and regulated differently. GLP-1s are genuinely well studied: tirzepatide produced average weight loss of 15.0% to 20.9% across doses over 72 weeks in SURMOUNT-1, versus 3.1% on placebo [6]. But the Wegovy label carries a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. Good evidence for one peptide doesn’t vouch for a completely different one, and GLP-1 safety still depends on a clinician screening you first.
How do I tell a real telehealth provider from a research-chemical seller at a glance? Look for the oversight layer: licensed physician review, a required prescription, compounded medications from licensed 503A pharmacies, and honesty that compounded isn’t the same as FDA-approved. Hiding who makes the product, or claiming a compounded version is identical to the approved drug, is exactly the marketing the FDA flagged when it warned 30 telehealth companies on March 3, 2026 [8]. FormBlends is one example of the accountable model done right, with HealthRX running the same playbook just behind it. Below that line sit the research-chemical retailers shipping vials marked not for human use.
Why does clinician screening matter this much? Because it catches problems a checkout page physically cannot, contraindications like the thyroid tumor history that rules out GLP-1s for some people [2], interactions with your current medications, and sensible titration instead of a five-compound starter pack. Skip the screening, skip that protection. And remember, price tells you nothing about safety, a suspiciously low price is a reason to look harder, not a reason to buy faster.
Is peptide therapy actually safe, or is that marketing spin?
Safety comes down almost entirely to sourcing and supervision. FDA-approved peptides used through a licensed prescriber and a verified compounding pharmacy carry a reasonable safety profile for most healthy adults. Research-chemical sources skip every quality-control checkpoint that would normally catch a problem. Even legitimate products can cause injection-site reactions, water retention, or hormonal shifts, so real medical supervision isn’t optional, it’s the whole point.
Does peptide therapy actually work, or is the science still catching up?
Depends entirely on the specific peptide and your goal. Semaglutide for weight management has solid clinical trial backing. BPC-157 and TB-500, popular in wellness circles, mostly have animal and anecdotal evidence, with human trial data still limited. Any claim that a peptide is a guaranteed fix is overselling what the science currently supports. A provider willing to spell out that distinction honestly is a better sign than one promising dramatic results.
What does peptide therapy typically cost, and what’s actually driving the price?
Costs range widely. A legitimate telehealth program with a physician consult, lab work, and compounded peptides often runs from a few hundred to over a thousand dollars monthly, depending on compound and dosing. What pushes the price up is real oversight, pharmaceutical-grade compounding, and follow-up care. Suspiciously cheap options usually mean those steps got skipped, and that’s exactly where risk climbs.
Where should I actually get peptide therapy, and how do I dodge the sketchy operators?
Go through a licensed telehealth physician who writes a genuine prescription, filled by an accredited compounding pharmacy. That accountability chain is the whole game. Supplement sites and research-chemical vendors operate entirely outside it, with zero obligation to verify purity or dosage. Some physician-supervised compounding services, FormBlends among them, are built specifically around that accountable structure. Checking a pharmacy’s PCAB accreditation or state board standing is a smart, free step before you spend a dime.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; McGuire and Fedoruk quotes; replication concerns. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022.
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023.
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, March 31, 2026.
Written by Lena Yang, health-industry reporter. Not a doctor, just a reader who chases the paper trail. Last reviewed March 2026.
Informational content only. Speak with a qualified healthcare provider about your own situation.